What Happens During a Menstrual Cycle?
The menstrual cycle consists of three phases: follicular, ovulatory and luteal.
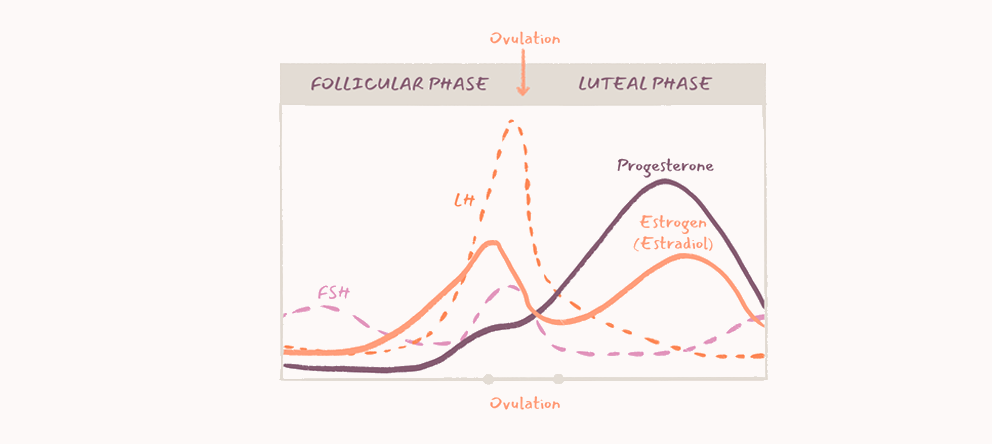
The follicular phase (average duration: 10 to 14 days)
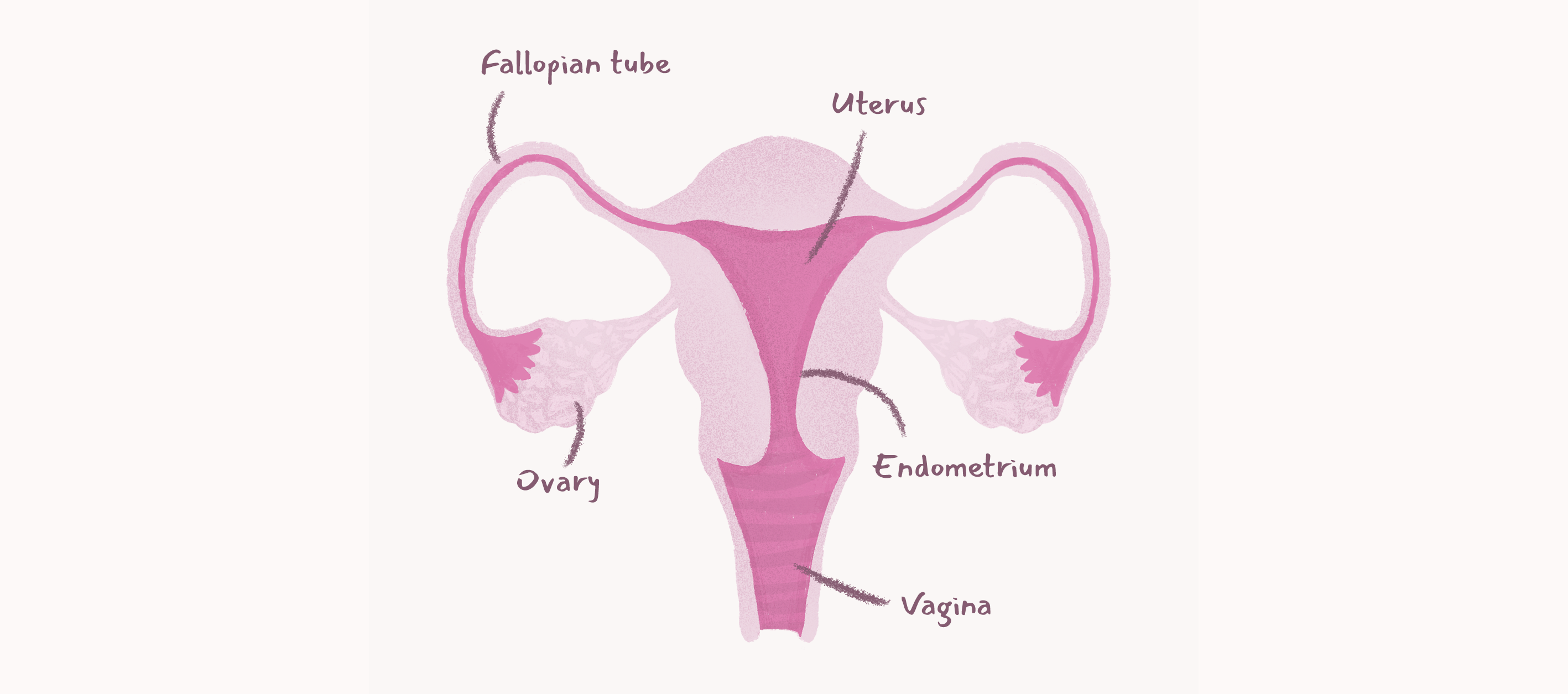
The follicular phase begins on the first day of menstruation and ends with a surge in LH (luteinizing hormone). During this phase, the hypothalamus (an organ located in the brain) produces gonadotropin-releasing hormone (GnRH) to stimulate the production of FSH (follicle-stimulating hormone). The FSH stimulates the growth of several follicles in the ovaries, but only one follicle will become dominant. The dominant follicle produces the hormone estradiol, which thickens the endometrium.
The ovulatory phase (average duration: 32 to 40 hours)
The rise in estradiol levels causes the pituitary gland to increase LH production: an LH surge begins and lasts between 32 to 40 hours, ending with the release of the egg (ovulation).
The luteal phase (average duration: 11 to 13 days)
Following the ovulation, the follicle that contained the egg becomes the corpus luteum, which produces the hormone progesterone. The latter prepares the endometrium for the implantation of the embryo and pregnancy. The egg travels to the fallopian tube after ovulation. If the egg is fertilized by a sperm in the fallopian tube, the embryo will be transported from the fallopian tube to the uterus 4 to 5 days after ovulation. Once in the uterine cavity, the embryo will attach to the endometrium for implantation. If there is no implantation, the levels of the estradiol and progesterone hormones decrease and menstruation begins.
For whom is induction of ovulation intended for?
Induction of ovulation is prescribed for women who are not ovulating or who have long and/or irregular cycles (> 35 days). Before starting medical treatment, the doctor must determine the cause of this ovulation dysfunction.
Some causes of the ovulation dysfunction: polycystic ovary syndrome (PCOS), low production of LH and FSH by the pituitary gland, ovaries that do not respond to LH and FSH hormones, thyroid disease, high level of the hormone prolactin (hyperprolactinaemia), obesity, eating disorders or extreme weight loss and / or exercise.
The doctor must also ensure, through additional tests, that there are no other reasons than the ovulatory dysfunction that explains a couple's infertility. He performs a test for the permeability of the fallopian tubes and a spermogram.
What are the treatments available for induction of ovulation ?
The cause of ovulation dysfunction will guide in choosing the appropriate treatment.
The most common ones are:
- Use of Metformin
- Use of Clomiphene
- Use of Letrozole
- Gonadotropins: FSH (follicle stimulating hormone), LH (luteinizing hormone), hMG (human menopausal gonadotropin)
- Use of GnRH (gonadotropin-releasing hormone)
- Use of ovarian drilling (or multi-perforation of the ovary)
- Weight loss
